996
Views & Citations10
Likes & Shares
Stevens-Johnson syndrome (SJS) and toxic
epidermal necrolysis (TEN) are severe, life-threatening
mucocutaneous disorder, with the adult incidence being estimated to be 0.4-1.2
cases/million; most commonly caused by drugs, with a high morbidity and
mortality that require immediate medical care. I hereby report a case of SJS
treated successfully with cyclosporine.
Keywords: Stevens-Johnson syndrome, Toxic epidermal necrolysis, Cyclosporine
INTRODUCTION
Stevens-Johnson syndrome (SJS) and toxic
epidermal necrolysis (TEN) are severe, life-threatening mucocutaneous disorder,
with the adult incidence being estimated to be 0.4-1.2 cases/million; most
commonly caused by drugs, with a high morbidity and mortality that require
immediate medical care [1]. Systemic corticosteroids have been utilized in the
management of SJS/TEN, but their use is still not universally accepted [2]. Cyclosporine,
intravenous gammaglobulin, cyclophosphamide, thalidomide or plasmapheresis has
been used in its treatment with varying success [1]. I hereby report a case of
SJS treated successfully with cyclosporine.
CASE PRESENTATION
A 59 year old
male, a known diabetic for 10 years, presented to us with painful,
erythematous, non-itchy rash over the face, back, buttocks and genital region
for 4 days, who subsequently developed fluid filled lesions and erosions,
redness and watering from the eyes, oral and genital ulcers within 24 h (Figure 1). The eruption followed
intake of paracetamol and diclofenac combination for pain in the legs. On
examination there were necrotic areas with sheets of epidermal detachment over
the face, back and buttocks; ocular examination revealed mucopurulent
conjunctivitis; genital region revealed confluent ulcers involving the glans,
shaft of penis and scrotum. Total body surface area involved was 35%.
Nikolsky's sign was positive. He was immediately admitted. His heart rate was
92 bpm, blood urea, 22 mg/dl, serum glucose, 283 mg/dl, serum bicarbonate, 24
mmol/L, haemoglobin 12.4 g/dl, total leukocyte count, 6300/cmm and total
platelet count 1.9 lac/cumm. There was no evidence of malignancy. A final
diagnosis of toxic epidermal necrolysis with a scorten of 3 was made. Apart
from the supportive care he was started on oralcyclosporine 100 mg twice daily
(3 mg/kg/day).
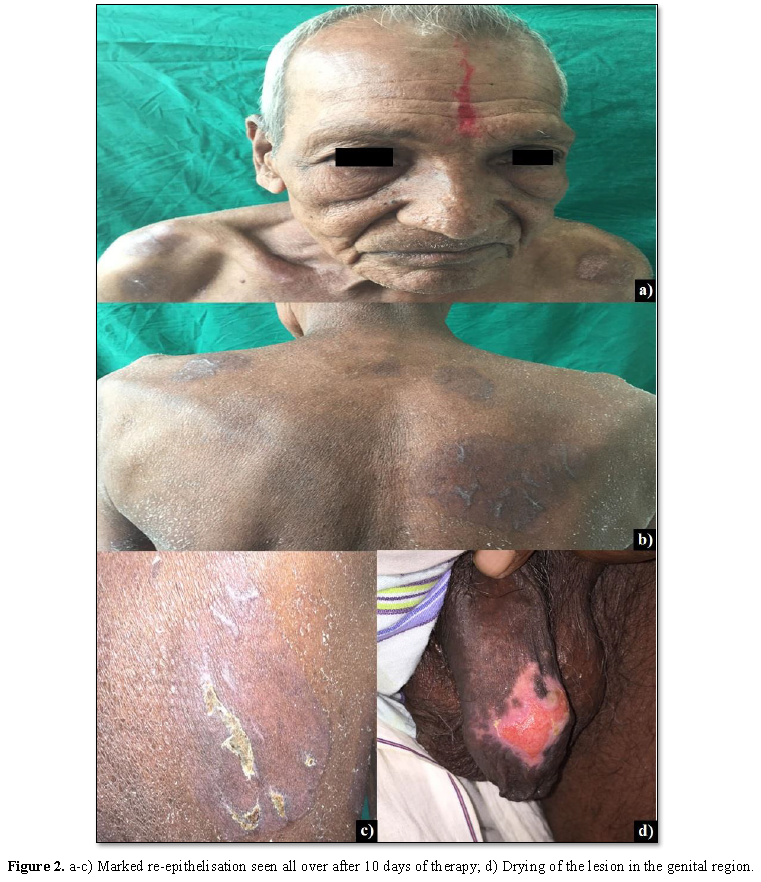
The patient showed marked improvement within 10 days of treatment (Figure 2).
DISCUSSION
SJS eponymously
named after Dr. Albert Mason Stevens and Dr. Frank Chambliss Johnson, who in
1922 first described cutaneous eruptions, severe ocular and oral involvement in
two young boys [3]. In 1956, Lyell introduced the term toxic epidermal
necrolysis [1]. In 1983, based on their similar histolopathologic findings, SJS
and TEN were synonymously associated with erythema multiforme major but later
Bastuji-Garin et al. in 1993 and Roujeau in 1994 proposed the differentiation
of erythema multiforme from SJS and TEN based on clinical and etiologic
information [3].
Majority of
cases are drug induced, high risk drugs being carbamazepine, phenytoin,
lamotrigine, olanzapine, ofloxacin, non-steroidal anti‑inflammatory
drugs, sulphonamide antibiotics and nevirapine; [1,3] while some cases have
been said to be triggered by infections the most common being mycoplasma
pneumonia [4]. The disease involves extensive necrosis of epithelial
keratinocytes of the skin and mucous membrane caused by cytotoxic T-lymphocytes
with the associated triggers being soluble as ligand, perforin and granzyme
[4].
CONCLUSION
Cyclosporine, a
calcineurin inhibitor, is frequently used in the treatment of organ transplant
and dermatologic conditions like psoriasis and atopic dermatitis. In SJS-TEN it
causes inhibition of inflammatory cytokines released due to activation of cytotoxic
T-cells and reduces keratinocyte apoptosis [5]. We present the above case to
display the effectiveness of cyclosporine alone without using corticosteroid in
the management of TEN.
1.
Sugunan
S, Kumar KKS, Sreenivasan P, Balachandran N (2017) Toxic epidermal necrolysis:
A study of clinical profile and treatment outcome in children. IJCH 4: 145-150.
2.
Law EH,
Leung M (2015) Corticosteroids in Stevens-Johnson Syndrome/toxic epidermal
necrolysis: Current evidence and implications for future research. Ann
Pharmacother 49: 335-342.
3.
Naveen
KN, Pai VV, Rai V, Athanikar SB (2013) Retrospective analysis of Steven Johnson
syndrome and toxic epidermal necrolysis over a period of 5 years from northern
Karnataka, India. Indian J Pharmacol 45: 80-82.
4.
Walsh S,
Lee HY, Creamer D (2016) Rook's Textbook of Dermatology. Wiley‐Blackwell, pp:
13-14.
5.
Conner
CD, McKenzie E, Owen CE, Callen JP (2018) The use of cyclosporine for
Stevens-Johnson syndrome-toxic epidermal necrolysis spectrum at the University
of Louisville: A case series and literature review. Dermatol Online J 24: 4.

QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Spine Diseases
- Ophthalmology Clinics and Research (ISSN:2638-115X)
- International Journal of Surgery and Invasive Procedures (ISSN:2640-0820)
- International Journal of AIDS (ISSN: 2644-3023)
- International Journal of Anaesthesia and Research (ISSN:2641-399X)
- Journal of Forensic Research and Criminal Investigation (ISSN: 2640-0846)
- Journal of Alcoholism Clinical Research


